| You are in category: DEFORMITIES |
«« back
|
Title: Genu valgum and post-traumatic ipometry:
correction with the Ilizarov method
Author: NUNZIO SPINA
| PICTURES |
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-
 -
-

|
The correction of the skeletal deformities of the limbs represents one of the elective applications of the Ilizarov method; moreover in comparison with other techniques or surgical instruments, it is said to be an exclusive way when a correction on more levels and at the same time the restoration of the normal length to be obtained.
More than as a simple external stabilizer of a correction already obtained surgically, the Ilizarov device acts, in fact, as a real �biological machine�, capable of modelling gradually the skeleton, subjected to the biological law of the distraction-compression and to the mechanical one of the hinges.
Biomechanical principles
A corticotomy performed at the apex of a simple angular deformity, with the axis of the hinges exactly perpendicular to the level of the deformity on the convex side (Fig. 1), enables to obtain, acting in distraction on the threaded rod on the opposite side, a progressive correction with the formation of a wedge of bone regenerate.
With the same process, but positioning the hinges at a certain distance from the skeleton axis (Fig. 2), a correction and a lengthening can be obtained at the same time, with the formation of a trapezoid-shaped regenerate.
Geometrically the hinges have to be, in a cutting section, on the perpendicular line of the diameter traced from the thrusting point: the latter has to be positioned connected with the four cardinal points, whether the deformity to be corrected in in varus, in valgus, in pro- or in re-curvatum (Fig. 3: correction of a valgus).
In case the angular deformity is on more levels (actually it is a false interpretation, because the deformity is always a single one), the thrusting point is placed more o less midway (Fig. 4: correction of a valgus-procurvatum).
In a post-traumatic deformity, the hinges are generally applied in the point of intersection of the axes of the bony segments concerned (and not at the level of the previous fracture) (Fig. 5): but in the distal region of the femur (where the mechanical and the anatomic axes do not coincide), the observance of this measure would bring about a correction of the mechanical axis with an alteration of the anatomical one (�golf club� deformity); in this case the point of intersection between the two axes, situated at the centre of the knee, will determine the correct position of the hinges: then a translation concealing the anatomic alteration is carried out (Fig. 6).
We have strictly taken into consideration these principles measures for the treatment, with the Ilizarov device, of a complex post-traumatic deformity (genu valgum and partially flexum, associated to ipometry) as a result a distal femoral fracture.
Medical case
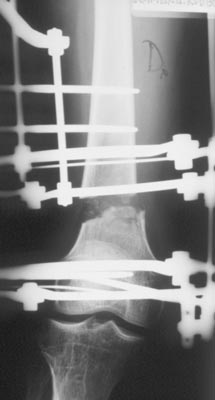
A 28 years-old man, with genu valgum of 25�, flexum of 8� and ipometry of 4,5 cm: result of malunion of a distal femoral fracture occurred at the age of 12. At the age of 16, unsuccessful attempt of correction of the deformity with osteotomy at the tibial level (Fig. 7 a, b: medical case and preoperating X-rays).
Operating technique
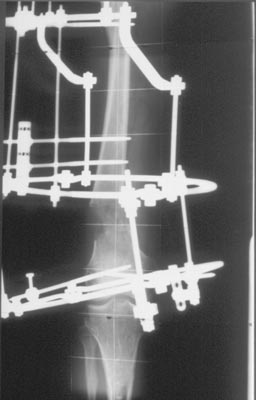
Treatment of the femur with the Ilizarov device: pre-assembly with 2 proximal arches and 2 distal rings, joined by rods of connection and oblique supports. Hybrid insertion: 2 half-pins respectively on the arches, 2 half-pins + 1 wire on the rings (Fig. 8), the position of the half-pins on the distal ring (Fig. 9) would avoid the entrapment of tendon-muscles strctures.
Corticotomy performed at 1/3 distal of the femur; connection between the two rings with three threaded rods, by applying the mechanic principles previously explained:
? the position of the thrusting point, that is of the �motor� rod, enables a correction mostly in varus, and partly in recurvatum to eliminate the flexum of the knee (Fig. 10);
? the hinges are in proximity to the knee, therefore under the distal ring, in order to avoid the formation of anatomic deformities (Fig. 6);
? the rods with the hinges, on the frontal side, are at a certain distance from the bone, so as to obtain a simultaneous lengthening (Fig. 6).
Post-operative care
The active motility of the hip and the knee, and the total weight-bearing with the crutches are granted immediately after the operation.
After one week, the beginning of the programme of lengthening and correction, managed by the patient himself. We have acted in distraction not only on the �motor� rod of thrusting, but also on the other rods, because of the entity of the initial shortening: mostly the rate has been of � mm x 3 a day on the lateral rod and of � on the two medial rods; short phases of slackening or compression have alternated according to the periodical clinical checks and to the tolerability of the patient.
The period of lengthening correction continued for a little more than 2 months.
The removal of the device has occurred after 5 months from the operation.
In the pictures 11 and 12 the clinical and radiographic situations respectively after 1 and 2 months (remark the correction of the flexum on picture 12 d, too).
Complications
Besides the usual drawbacks connected to the pain and to the cutaneous intolerance, the major problem has been represented by the stiffness of the knee: surely not all the possible preventive measures have been put into effect, such as the fact of practising with a bistoury partial release of the muscular fascia, before introducing tha half-pins on the distal ring, and before verifying immediately the possibility of free articular movement: moreover, we have not insisted enough, during the initial post-operative phase, on the recovery of the active motility.
Such stiffness has demanded a long and intensive physiotherapy, wich has given its results only several months after the removal of the device.
Result
Good correction of the deformity, both on the frontal and on the sagittal side, and complete restoration of the length (Fig. 13 a, b); one year after the operation, satisfying recovery of the articular movement of the knee, from 0� to 100� (Fig. 14).
The patient came back, without any limitations, to his job as an electrician.
Conclusions
The Ilizarov treatment is a �biological machine� wich has considerable potentialities in the correction of any type of skeletal deformity (in particular in the long bones of the limbs) and of the simultaneous restoration of the normal length. Beyond the various measures of the technique, the fundamental premise for a good clinical result is represented by a detailed pre-operating geometrical study, by taking into consideration the axis of reference and the correct application of the hinges.
Bibliography
1) Catagni MA, Villa A, Guerreschi A
Theoretical and practical basis for a correct application of Ilizarov in the fractures, pseudoarthrosis, lengthening, deformities.
Divisione di Ortop. e Traum.Ospedale di Lecco - Italy
2) Catagni MA, Cattaneo R, Villa A
Correction of angular deformities about the knee
In: Operative Principles of Ilizarov
Milano: A. Bianchi Maiocchi and J. Aronson 1991, pp. 413-30.
3) Catagni MA, Malzev V, Kirienko A
Femoral correction og genu-valgum.
In: Advances in Ilizarov apparatus assembly
Milano: A. Bianchi Maiocchi 1994, pp 102-4.
|